







1 MOTOR LEARNING FOR STROKE PATIENTS AFTER THE FUNCTIONAL ELECTRICAL STIMULATION IN KNEE HYPEREXTENSION MODEL WINAI CHATTHONG A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ENGINEERING (BIOMEDICAL ENGINEERING) FACULTY OF GRADUATE STUDIES MAHIDOL UNIVERSITY 008 COPYRIGHT OF MAHIDOL UNIVERSITY 2 3 4 ACKNOWLEDGEMENT I would like to express my sincere gratitude and deepest appreciation to Dr.Zeng Lertmanorat, my principal advisor who always supervises me with excellent knowledge, valuable advice, constant encouragement and support, proof reading of this manuscript, and all problems solving throughout the study including financial support. The equally grateful and deepest appreciation also goes to Assistant Professor Vimonwan Hiengkaew, my co-advisor for her great wisdom, thoughtful guidance, useful knowledge of statistics, proof reading of this manuscript and all problem solving in this study. Additionally, I would like to express my deepest appreciation to Dr.Supalak Khemthong, for his invaluable advice and excellent constructive comments in this research. I would like to thank greatly with gratefulness to Miss Kanitta Jittree and Physical therapists at the clinic of the Faculty of Physical Therapy and Applied Movement Science for their assistance and permission to recruit subjects for the study with warmest support and helpfulness. I would like to give thankfulness to all my subjects for their good participation. Finally, I would like to express my infinite gratitude to my parents for their love, unending care, understanding, warmest encouragement, assistance as well as financial support. The usefulness of this thesis, I dedicate to my mother, my father and all the teachers who have taught me since my childhood. Winai Chatthong 5 Fac. of Grad. Studies, Mahidol Univ. Thesis / iv MOTOR LEARNING FOR STROKE PATIENTS AFTER THE FUNCTIONAL ELECTRICAL STIMULATION IN KNEE HYPEREXTENSION MODEL WINAI CHATTHONG EGBE/M M.Eng. (BIOMEDICAL ENGINEERING) THESIS ADVISORS: ZENG LERTMANORAT, Ph.D. (Biomedical Engineering) VIMONWAN HIENGKAEW, Ph.D. ABSTRACT This study compared the effectiveness of three rehabilitation training programs on motor recovery for stroke patients in knee hyperextension model including 1) manual facilitation, ) electrical stimulation with massed practice (ESm), and 3) electrical stimulation with distributed practice (ESd). Twenty-four stroke subjects with comparable conditions were assigned randomly to one of the three groups. The control group received standard manual facilitation rehabilitation for 60 minutes. Both ES groups received the same 30-minute standard rehabilitation as the control group. The ES training was then applied for 30 minutes by stimulating the hamstring muscle to help patients elicit the knee bending. ESm included 5 sets of 5-minute training with 1-minute rest. ESd includes 3 sets of 5- minute training followed by 5-minute. All subjects received training 3 times a week for a total of ten times. Knee control was evaluated by measuring the knee angles during standing and walking, and response time. Esd training program improved the knee control significantly more than did either the control or ESm group. Knee angles of ESd group during standing decreased from to , compared to those of control group from to , and ESm group from to Response time for ESd group also significantly decrease from to , whereas those of control and ESm groups improved from and to only and , respectively. Whereas those the ESd group produced a significantly higher increase of the performance of knee angle and response time with respect to the control and the ESm group (p<0.05). KEY WORDS: MOTOR RECOVERY/ ELECTRICAL STIMULATION/ STROKE/ KNEE HYPEREXTENSION 74 pp. 6 Fac. of Grad. Studies, Mahidol Univ. Thesis / v การศ กษาว ธ กระต นไฟฟ าเพ อฟ นฟ ผ ป วยโรคหลอดเล อดสมองโดยใช อาการเข าแอ น (MOTOR LEARNING FOR STROKE PATIENTS AFTER THE FUNCTIONAL ELECTRICAL STIMULATION IN KNEE HYPEREXTENSION MODEL) ว น ย ฉ ตรทอง EGBE/M วศ.ม. (ว ศวกรรมช วการแพทย ) คณะกรรมการควบค มว ทยาน พนธ : เซง เล ศมโนร ตน, Ph.D. (Biomedical Engineering) ว มลวรรณ เห ยงแก ว, Ph.D. บทค ดย อ การศ กษาคร งน ม ว ตถ ประสงค เพ อศ กษาผลกระทบการเร ยนร ควบค มห วเข าโดยใช เคร องกระต นไฟฟ ามาประย กต ร วมในการฝ ก โดยทดสอบว ากล มท ฝ กด วยว ธ ทางกายภาพบ าบ ดเพ ยง อย างเด ยว (ควบค ม) ก บกล มท ฝ กด วยว ธ กระต นไฟฟ าในช วงกระต นนานช วงพ กส น (ESm) และช วง กระต นก บช วงพ กเท าก น (ESd) กล มไหนจะท าให ม มของห วเข าและการตอบสนองในการงอเข าด ข น ในการศ กษาคร งน กล มต วอย างค อผ ป วยอ มพาตคร งซ กท งหมด 4 คนท ม ล กษณะใกล เค ยง ก น โดยจะแบ งด วยการส มออกเป น 3 กล ม ค อกล มควบค ม กล ม ESm และกล ม ESd กล มละเท าๆก น โดยกล มควบค มจะได ร บการฝ กจากน กกายภาพเพ ยงอย างเด ยวตลอด 60 นาท ในขณะท กล มท เหล อ จะได ร บการฝ กจากน กกายภาพ 30 นาท หล งจากน นก จะมาฝ กโดยใช เคร องกระต นไฟฟ าอ ก 30 นาท กล มต วอย างท งหมดจะได ร บการฝ ก 3 คร ง/ส ปดาห จนครบ 10 ว น ม มของห วเข า การตอบสนองการ งอเข า จะเป นค าท น ามาประประเม นถ งความสามารถในการควบค มห วเข า ซ งค าด งกล าวจะถ กว ดก อน ฝ ก ท นท หล งฝ ก 15 นาท หล งฝ ก และ หล งจาก 4 ช วโมงหล งฝ กในคร งส ดท าย หล งจากฝ กพบว ากล ม ESd ม ความแตกต างในเร องม มของห วเข า การตอบสนองการงอของ ห วเข า ท ด กว ากล ม ESm และกล มควบค มอย างม น ยส าค ญทางสถ ต (P<0.05) และย งพบว าช วง 5 คร ง ส ดท ายของการฝ ก หล งจากท พ ก 15 นาท กล ม ESd ม ความคงความสามารถในม มของห วเข าและเวลา ในการตอบสนองได ด กว ากล ม ESm และกล มควบค ม ล กษณะท ด กว าในกล ม ESd บอกได ว าการกระต นไฟฟ าแบบท ม ช วงกระต นเท าก บช วงพ ก เม อน ามาใช ร วมก บการท ากายภาพบ าบ ดสามารถท าให เก ดการเร ยนร การเคล อนไหวได ซ งให ประส ทธ ภาพท ด กว าการท ากายภาพบ าบ ดเพ ยงอย างเด ยว การฟ นฟ ท น าเคร องกระต นไฟฟ ามาร วมใน การฝ กจ งเป นแนวทางท จะแก ป ญหาการเด นเข าแอ น และน าสนใจท จะน าไปศ กษาต อ เพ อควบค ม ส วนอ นๆของร างกายในผ ป วยอ มพาตคร งซ กต อไป 74 หน า. 7 CONTENTS Page ACKNOWLEDGEMENTS iii ABSTRACT iv LIST OF TABLES viii LIST OF FIGURES ix LIST OF ABBREVIATIONS x CHAPTER I INTRODUCTION 1 II OBJECTIVE 5 III LITERATURE REVIEW 6.1 Stroke and knee hyperextension 6. Motor recovery 7.3 Electrical Stimulation 14 IV MATERIALS AND METHODS Participants Training procedures Assessment procedures Statistical analysis 4 V RESULTS Immediate effect of ES training on knee angle and 5 response time 4. Overall improvement after completing the training 30 8 vii CONTENTS (Continued) Page CHAPTER VI DISCUSSION 34 VII CONCLUSION 37 VIII CLINICAL RELEVANCE AND FURTHER STUDY 38 REFERENCES 39 APPENDIX 50 BIOGRAPHY 74 9 LIST OF TABLES TABLE Page 3.1 Characteristics of subjects 17 D.1 Mean and standard deviation of control and ES groups at 1 st training 6 D. Mean and standard deviation of control and ES groups at nd training 6 D.3 Mean and standard deviation of control and ES groups at 3 rd training 63 D.4 Mean and standard deviation of control and ES groups at 4 th training 63 D.5 Mean and standard deviation of control and ES groups at 5 th training 63 D.6 Mean and standard deviation of control and ES groups at 6 th training 64 D.7 Mean and standard deviation of control and ES groups at 7 th training 64 D.8 Mean and standard deviation of control and ES groups at 8 th training 64 D.9 Mean and standard deviation of control and ES groups at 9 th training 65 D.10 Mean and standard deviation of control and ES groups at 10 th training 65 E Angles measured between two segments 66 F.1 The knee angle was measured on three consecutive days 68 F. The response time was measured on three consecutive days 68 F.3 Intratester reliability of the knee angle calculation and response time 68 G.1 Knee angle during walking between pre-training, post-training in 69 control and training groups, massed and distribute practice (Positive knee angle represents knee flexion and negative angle indicates knee extension) G. Knee angle during walking after knee flexion between pre-training, 70 post-training in control and training groups, massed and distribute practice (Positive knee angle represents knee flexion and negative angle indicates knee extension) G.3 Response time between pre-training, post-training in control and 70 training groups, massed and distribute 10 LIST OF FIGURES FIGURE Page 3.1 Preparation of training Flowchart of the training programs The assessment diagram 3.4 The position of marker 3.5 The top view of camera and walkway in this study Location of markers and knee angle in the sagittal plane Knee angle during standing after knee flexion (degrees) of the 6 control and ES groups in each 10 assessments 4. Knee angle during walking in the midstance phase (degrees) of the 7 control and ES groups in each 10 assessments 4.3 Response time during standing in knee flexion (s) of the control 9 and ES groups in each 10 assessments 4.4 Arithmetic series of response time (s) of the control and ES groups 30 in each 10 assessments 4.5 Mean comparison of knee angle and response time between control 31 and ES groups 4.6 Percent-change comparison knee angle and response time between 33 control and ES groups 11 LIST OF ABBREVIATIONS Ө = angle AFO = ankle foor orthosis CVA = cerebrovascular accident FES = Functional electrical stimulation ESd = Electrical Stimulation with distributed practice ESm = Electrical Stimulation with massed practice KH = knee hyperextension KP = knowledge of performance KR = knowledge of result KSa = knee angle during standing KW = knee angle during walking m = meter (s) min = minute (s) MRP = motor relearning programme n = number of subject No = number PNF = proprioceptive neuromuscular facilitation ROM = range of motion RT = response time sec = second (s) TSME = Thai mental state examination 12 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 1 CHAPTER I INTRODUCTION Stroke also known as cerebrovascular accidents (CVAs) is a leading cause of adult disability [1]. This pathology affects the neurology of the human body and causes hemiparesis or hemiplegia [, 3]. In 005, World Health Organization estimated that stroke resulted in 5.7 million deaths and indicated that the number of stroke patients will continue to rise [4, 5]. Stroke is also a leading cause of death and long-term disability in Thailand [6]. The type of CVAs can be divided into the ischemic and hemorrhagic CVAs [7, 8]. Stroke type does not influence on recovery of walking ability []. Stroke-survival impairment depends on the location and severity of lesion [9], including perception, cognition, muscle strength, motor control, speech, active mobility, disturbance of sensory, tone balance, and psychological function []; thus leading to a poor quality of life. Rehabilitation is necessary in enhancing functional abilities of hemiplegic patients. The goal of the motor rehabilitation is to assist patients regain the motor control of the body. Motor control and motor recovery will lead to enhance these activities, which is the vital capability that all stroke patients can develop. Motor recovery is a process that involves the effect of repetitive movement [10] which leads to the improvement in competence of skill action [11-14]. The early period of repetitive practice [13-15] can changes the immediate performance. It always apply for motor recovery in stroke patients [16-18]. 13 Winai Chatthong Introduction / Several researchers in the field of neurorehabilitation have advocated using massed or distributed practice in motor recovery [19]. Massed practice is defined as a continuous practice with either no rest at all or very short rest intervals during practicing [0]. Distributed practice means a regime in which periods of training are interspersed with rest periods or spacing these intervals of work apart with longer periods of rest [1]. Massed practiced has been widely used in rehabilitation. It is also known as constrain induce movement therapy []. Although tasks under massed practice may increase competence at the early trials but without solid advantage for learning [11, 0, 1]. Distributed practice has been used less often than massed practice because it requires long time periods in course training [11]. Nevertheless, distributed practice can retain the performance if patients accomplish learning [1]. One of the major disabilities following stroke is gait impairment. The impairments have significant effects upon walking ability. Truthfully, around percent of hemiplegic patients regain their walking ability independently at 3 weeks after discharge [3]. Although, patients walk independently but they demonstrate impaired walking function. Around half of these are not able to walk even with personal assistance [4]. Hence, rehabilitation is important to enhance the functional abilities of stroke patients. Knee hyperextension (KH) is one of the major problems in gait training [4]. More than half of patients with hemiparesis have KH in stance phase [5]. In this phase, the knee joint is normally in a slightly flexed position approximately 5 degrees [6, 7]. On the other hand, KH in hemiparetic patients has been distinctly shown locking the knee during walking in midstance phase of gait cycle. The body compensates for the tight hip extensors by extending the knee [4, 7]. There are several causes for KH in stroke patients, for example, 1) poor control over the knee joint due to impaired muscle tone; quadriceps spasticity, plantar flexor spasticity ) poor control over the knee joint due to muscle weakness, such as 14 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 3 hamstring and quadriceps weakness 3) coordination impairment of knee flexor and extensor muscles and 4) joint proprioceptive impairment [11, 8, 9]. KH results in several deteriorating effects such as the quality of gait [30] and altered cosmetic of gait that may affect the patient s life style [7, 31-33]. KH also contributes to joint damage, deteriorating, instability and pain in long term. Additionally, it may also cause gradually stretch joint capsule owing to the increasing force impact on knee joint during walking [7, 34]. Several techniques have been used for KH management. These techniques are divided into two groups by rehabilitation intervention. The first group is the manual facilitation [11]. It is Proprioceptive Neuromuscular Facilitation (PNF) [35], Bobath [36] and exercise [37]. The second is specific clinical equipments. This technique includes knee ankle foot orthoses (KAFO) [38], electrical stimulation (ES) [9, 30, 31, 39, 40]. In manual facilitation, PNF can be applied to improve quadriceps and hamstrings muscle control and relearning [35]. In addition, the manual resistance from rehabilitation teams or resistance from pulleys and resisted bands can be used to stimulate these muscles control [37, 41]. There is also one important technique as a Bobath. It is usually applied to prevent the hyperextended knee in early recovery and exercise in weight bearing with control movements of knee. This technique begins with small isolated movements [4]. The effectiveness of manual facilitation is usually humbled by the limited train period. Commonly manual facilitation techniques require an interaction between the therapist and the patient. The therapy can be provided only for a short period of time daily [43]. The duration of treatment is the most important factor that effects the efficacy of rehabilitation [11]. Therefore, the rehabilitation management should consider the ability of patients, and therapists should encourage the patients to practice independently for promoting the efficiency of learning and recovery [37, 44]. 15 Winai Chatthong Introduction / 4 For clinical special equipment technique, orthosis device is able to decrease the knee hyperextension caused by plantar-flexor muscle hyperactivity and quadriceps muscle weakness. KAFO could be applied to increase stability and knee hyperextension limitation [38]. Previous research [45] suggested the use of Swedish knee cage for management of KH in hemiplegic patients. After removed from hospital, nine patients had all gained active knee control, and hyperextension was no longer a problem. One of the most disadvantages is that it is uncomfortable and hard to wear. In addition, KAFO has a limited range of motion in several joints which can cause the pressure sore [46]. ES has been widely used in rehabilitation for training stroke patients [39, 40, 47]. ES aims to generate movements or functions which mimic normal voluntary movements, and also to restore the functions when movements serve. ES has been applied in the restoration of foot drop, standing and walking [40, 48]. ES can be used to enhance gait pattern in stroke patients who have abnormal muscle tone in the leg [39]. ES in rehabilitation has been applied, mainly based on massed practice. That is, movement practice is often repetitive and consecutive during task with minimal rest period. It is believed that muscle strength and power is immediately improved after training by FES [40]. However, this process may not be the most efficient way of motor recovery [1]. A strong suggestion of motor recovery research challenges the notion that distributed practice may be a more effective way to improve motor actions [10, 49, 50]. 16 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 5 CHAPTER II OBJECTIVE The objective of this study was to investigate the effectiveness of electrical stimulation (ES) training programs on motor recovery improvement for stroke patients. ES training with mass (ESm) and distributed (ESd) practice programs were carried out and its effectiveness was compared to traditional manual facilitation. The study was performed on KH model as one of the major problems in gait training. The outcome of this study could provide a useful guidance for planning a suitable training program for KH in hemiparetic patients with regards to management at clinical rehabilitation of post-acute stroke patients. 17 Winai Chatthong Literature Review / 6 CHAPTER III LITERATURE REVIEW.1 Stroke and Knee hyperextension Commonly observed gait deviations in the stroke patient are plantar flexion (equines), plantar flexion and inversion (equinovarus), excessive knee extension (genu recurvatum), and inadequate knee flexion during swing (stiff knee gait) [9]. Knee hyperextension is one of the gait adaptations in stroke patients [3] that usually develops during mid-stance into terminal stance of gait cycle [5, 30]. Fifty-seventy percent of hemiparetic patients suffer from knee hyperextension [5, 31]. It is associated with muscle conditions such as hamstring and quadriceps muscles weakness [5, 9], quadriceps muscles spasticity [33], spasticity or contracture of ankle plantarflexor muscles [11, 8] and knee flexor muscles weakness [51, 5]. Recovery stages of Stroke patients are divided into 1) flaccid stage, ) spastic stage and 3) rate recovery stage based on pathophysiological mechanism [8]. Recovery process takes place in two means: natural neurological recovery and rehabilitation to improve motor recovery skill [9]. Both recoveries concern several factors that influence recovery of functions such as initial stroke severity, cognitive impairment, serious systemic illness, age, gender, and types and sides of stroke [53]. For the rehabilitation, a physical therapist helps patient exercising in order to recover and maintain motor functions [54-56]. The objective of exercise is to improve the muscle strength and endurance [57]. In general the effectiveness of exercise depends on the level of exercise resistance [54-56], number of repetitions and sets [37, 43, 54]. 18 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 7 The ultimate goal of neurorehabilitation is not only to facilitate the muscle strength and endurance, but also to recover the motor control. Motor recovery is important to the rehabilitation of patients with hemiplegia. It can imply recovery function movement in stroke [0, 1].. Motor recovery Motor recovery is the capability of the acquisition and modification of movement [11, 1]. It relates recovery process. There are four attributes essential to recovery. First, recovery is a process of acquiring the capability for producing skilled actions. Second, recovery comes from practice or experience. Third, recovery is based on behavior and cannot be reconnoitered directly. Fourth, recovery produces permanent changes in behavior [11, 0]...1 Stage of motor recovery There are three main stages concerning of motor recovery; cognitive, associative, and autonomous phases [10, 1, 50, 58, 59]. In cognitive stage of motor recovery, patient must engage in cognitive activity as they listen to instructions and receive feedback from the therapist. The instructions and visual feedback are most effective during this phase [1]. In the associative stage, patents learn to associate certain environmental cues with the movements required to achieve the goal of the skill. They make fewer gross errors and approach maximum efficiency for doing the task. Proprioceptive feedback is important in this phase. Furthermore, repetitive practice is necessary in this phase. Also during this stage, patients acquire the capability to detect and identify some of their own performance errors [1]. 19 Winai Chatthong Literature Review / 8 After intensive practice and experience, some patients turn into the autonomous stage when patients perform task with low degree of attention or do not consciously think while performing the skill. Patients can begin to devote attention to other aspects of the skill or focusing on the secondary task. Additionally, these skilled performers can detect their own errors, and make the proper adjustments to correct them. Performance becomes consistent... Factors affecting motor recovery Factors that influence motor recovery consist of practice, repetition, feedback, and contextual interference [37, 60-63]. These factors are important to help patients overcome their deficits [1]. a. Practice One of the most effective ways to improve motor recovery is to practice [1]. Practice changeability refers to the variety of context characteristics that the learner experiences while practicing a skill. Also variability in practice is essential for motor recovery. The amount of practice is considered to be the strongest influence on motor recovery [10, 1]. Recovery resulted from practicing leads to the improvement on capability of skill action in short-term and long-term functional changes [11, 14, 64]. The effect of a long-term practice contributes to the development of a long-term functional change of motor recovery [11, 65]. Indeed, it is also helpful to know what practice conditions support and optimize recovery, so that therapy sessions can be structured to maximize the patient s recovery. Practice in stroke rehabilitation is divided into physical practice [11, 1, 63] and mental practice [1]. Physical practices Physical practice is the act of performance in recovery and obtaining experience. Physical practices are catergorized into several aspects such as massed versus distributed, constant versus variable and random versus blocked [11, 1, 63]. 20 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 9 Massed practice, also known as constraint-induced movement therapy technique [18, ], is defined as a continuous practice with no rest period or as a practice session in which the practice time is longer than the rest period between practices. Massed practice approach has been widely used in the upper limb training for patients with chronic vascular accidence or chronic traumatic brain injury [, 44]. Previous study [66] applied the constraint induced movement therapy in chronic stroke patients for improving the dexterity in hand. Patients improved their hand function better than did the control group. Additionally, massed practice was also applied on the balance recovery training in cerebral palsy for 5 days [67]. The result showed significant improvement of stability by reducing center of pressure area and time to stabilization after training. Distributed practice is defined as practice interspersed with long resting duration between practice sessions [0]. Although massed practice increased immediate accomplishment in motor recovery better than distributed practice [1, 63], a previous study showed that distributed practice was significantly better than massed practice in terms of a task performance and a long term retention [17]. Constant practice involves practicing the same movement task in the same way for every trial. It is appropriate for tasks that require minimal variation. Variable practice involves altering the conditions of the task across practice trials. It is appropriate for tasks that are likely to be performed in variable condition. Variable practice appears to be more effective in motor recovery than constant practice [68]. Blocked practice is defined as practicing one task for a block whereas random practice is defined as practicing more than one task for a block of trials then moving on to the next task. Random practice may be inappropriate until patients understand the dynamics of the task. Blocked practice is appropriate for the patient to begin with practicing one skill repeatedly. This is not long-term recovery and the ability is limited. In contrast, encouraging the patient to practice a number of tasks in random order may slow down the initial acquisition of skills but is better for long-term retention on motor recovery [11]. 21 Winai Chatthong Literature Review / 10 Mental practices Mental practice usually involves imaging oneself performing a skill in order to promote motor recovery. It relates to the recovery and performance of skill motor recovery [1]. Mental practice is usually combined with physical practice unless patients cannot perform the physical practice [11]. Moreover, during mental practice the brain induces plasticity in the motor cortex area such as muscular imagined, cortical motor evoked potential, and cerebral blood flow in neuromotor pathways [60, 69]. b. Repetition The repetitive movement is essential for improving skilled movement in motor recovery. Rehabilitation uses repetitive practice for training stroke patients to increase muscle strength, improve performance and regain muscle coordination. Several studies suggest that stroke patients should practice thousands of times in order to restore loosed motor program, gain a volitional motor control sequence, and develop an optimal way for performing the movement [43]. Repetitive quality of the knee control should be slow and smooth movement during practice. Repetitive practice is able to apply with functional closed kinetic chain promoting the neural ability to recruit groups of knee muscles to work together [1]. In addition, it creates neural pathway that closely replicates the demands of activity in order to develop a new movement recovery process [70]. Therefore, the posture of this training could activate knee motor recovery in patient with knee hyperextension. Several studies [64, 65, 71-73] indicated that repetitive training could improve motor cortex plasticity, especially physical therapy techniques used in stroke rehabilitation. Butefisch in 1995 [6] applied a repetitive training on movement of the affected hand in stroke patients. Training consisted of repetitive hand and finger flexions and extensions against various loads. After therapy, they found improvement of specific movement parameters of the hand, such as grip strength, peak force of isometric and peak acceleration of isotonic hand extension. These results indicated an improvement of motor recovery during training. 22 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 11 Although, repetitive training can promote motor recovery. The effects of rehabilitation are often limited by duration of treatment because the patients need to relearn around thousands of repetition [43]. Moreover, strengthening of quadricep and hamstring muscles are usually done by using an individual exercise program practice to thousands of repetitions [43, 74]. Patients may be discomfort because of muscle fatigue [54]. Some studies indicated that repetitive stimulations of the sensorimotor system during a long period exercise have probably influenced on a decline in postural or gait control [75]. These changes may have an impact on gait velocity alteration. c. Feedback Feedback is the information that the patient receives about the performance while recovery a skill or a new performance [0, 37]. Feedback information can be further derived from intrinsic and extrinsic sources, both of which are essential for increasing the rate of improvement on new tasks, enhancing performance on task movement [76] and improving a motor recovery[1] Intrinsic feedback is the sensory feedback available during or after a person has performed a skill that is a naturally occurring part of the skill performance situation itself [1]. Sensory integrations contribute to improving feedback information. This individual sensory system consists of proprioception, tactile, vestibular, visual, and auditory sensory system [11, 37]. All of the sensory information are necessary for the error-detection process in the nervous system. However, stroke patients who have the reduction of sensory input will be limited in receiving the intrinsic feedback [1]. Therefore, the supplementary of sensory stimulation has become an important role to the nervous system [63, 76]. Extrinsic feedback, also known as augmented feedback, is the information that receives from external sources including feedback from therapist or equipments, such as EMG biofeedback, videotape, or data information from kinetic and kinematic analysis. This feedback is the supplementary for intrinsic feedback [11]. External feedback is divided into knowledge of result [77] and knowledge of performance (KP). 23 Winai Chatthong Literature Review / 1 The improvement of motor recovery must combine these two types of knowledge of result and knowledge of performance [1, 37]. Knowledge of result (KR) is the form of feedback provided with the outcome of the skill acquisition. It provides information about errors, thus giving the learner information about whether to modify the movement on the next attempt [11]. Previous researches indicated that the less feedback frequency during training tended to be more advantage for long term in the retention and transfer phase whereas providing immediate KR and more feedback frequency tended to improve particularly performance during the acquisition phase [11]. These results suggested that the therapist should limit the frequency and immediacy of KR feedback during rehabilitation to improve motor performance and recovery in stroke patient [10, 1]. Knowledge of performance (KP) is verbal post action information feedback about the correctness of the movement pattern that the patient has made. It provides information about the processes of movement pattern which the patient uses during task performance. Commonly, instruction and suggestion during practice enhance the knowledge of performance [63]. Biofeedback is a technique usually used in improving knee control. Controlled trials on stroke patients have shown that movement related specific feedback led to a clinically significant improvement and was better than traditional exercise programs [31, 78]. Koheil in 1980 [79] studied the effect of joint position biofeedback in gait training. The results of this case study emphasized the potential usefulness of joint position biofeedback as a part of the total physical therapy approach to gait training in hemiplegic patient. Hogue in 1983 [31] used auditory biofeedback treatment for patients who had knee hyperextension. Comparison of subjects before and after auditory biofeedback training showed the decrease in knee hyperextension after auditory biofeedback in all subjects. Morris in 199 [30] studied the effect of electrogoniometric feedback on knee hyperextension in 6 stroke patients. These results suggested that the addition of electrogoniometric feedback to standard physical therapy enhanced the effectiveness of treatment for knee hyperextension in stroke. 24 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 13 Dursun in 004 [80] used a special universal electronic genu recurvatum biofeedback system to prevent knee hyperextension. It was similar to the studies of Koheil and Hogue [31, 79]. However, this type of goniometer had its drawbacks because the device itself must be placed across the knee so it tends to limit the patient s walking ability. Although bio-feedback training and manual facilitation have been used to improve motor recovery in stroke patients, they still have some restrictions. Bio-feedback training should be performed during the execution of an actual movement of interest (locomotion) rather than training the patients to control the activation of the muscle during isolated movement of the joint [11]. Most of the studies on bio-feedback have been restricted to training subjects to regulate the level of activation [81]. Additionally, the results did not improve in gait velocity and singlelimb stance times [30]. d. Contextual interference The contextual interference is one of the effects in skill motor recovery, several suggest that variation of context will improve the motor recovery and facilitate other types of movement performance in nearly normal pattern [11, 1, 76]. Contextual interference labels the interference resulting from practicing a task within the context of the practice situation. A high degree of contextual interference can occur when a patient practices several different but related skills during the same practice session [1]. 25 Winai Chatthong Literature Review / 14.3 Electrical Stimulation (ES) Electrical stimulation (ES) or neuromuscular electrical stimulation (NMES) is a method of applying electrical currents to the body in order to enhance or restore function [39]. Three electrode types have been extensively used including a surface, percutaneouse and implant electrodes [48]. ES has been studied and used for paraplegic patients due to stroke, spinal cord injury (SCI), multiple sclerosis (MS), brachial plexus injury, and traumatic brain injury [40, 48, 8]. ES has been used in stroke rehabilitation since early nineteenth century [83]. It was applied in the clinical rehabilitation for diagnosis, therapeutic and functional recovery. The primary goal of ES is able to restore sensation, skeleton motor function and autonomic function in physical impairment [48]. There was important advantage of this for motor recovery. It directly stimulates a muscle [40] by repetitive movement therapy [39]. The rehabilitation of ES was divided into upper and lower limb. According to the upper extremities, ES could provide the hand function movement for individuals with stroke. Several reports used ES for replacing grasp and release function [84, 85] and promoting muscle power on shoulder [86] in stroke. Additionally, previous research applied ES for reducing spasticity on the upper limb [87]. According to lower limb, initial application of ES in stroke patients focused on gait enhancing. Dependence in walking is one of the primary goals for stroke rehabilitation patients. Approximately 35 % of survivors with stroke do not regain useful walking function and 5 % of all recruits from stroke are unable to walk without full physical assistance [88]. Thus, gait training by ES accounted for a large proportion of time spent in stroke rehabilitation [39, 89]. The applications of ES are successful in rehabilitation gait restoration. 26 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 15 ES can provide gait restoration during swing phase of gait cycle [90] in stroke patients. After 3 weeks of treatment, patients were able to walk [83]. Several ES was applied to 4 muscles in the lower limbs [91, 9] in order to promoting gait sequence. Additionally, ES has been extensively used in foot drop [93]. This may result in stumbles, fall and using more energy while walking. Furthermore, the application of therapeutic exercise with ES could improve bilateral control in stroke [94] and reduced the time needed to recovery [8, 95]. 27 Winai Chatthong Materials and Methods / 16 CHAPTER IV MATERIALS AND METHODS 3.1 Participants Twenty-four hemiparetic patients with KH were participated in the study with age range between 30 and 70 years. All subjects were informed about objectives, process of testing and training. Subjects signed a statement of informed consent prior to participating in this study (Appendix B). The study was approved by Ethical committee for Human subject research, Mahidol University. The medical inclusion and exclusion criteria for patient selection were as follows Inclusion criteria - Having first onset of stroke. - Post stroke at least 3 months. - Adequate stability at the hamstring muscles during stance with stimulation - Ability to walk independently at least 10 meters without using assistive devices. - Having knee hyperextension during mid-stance phase of gait. - Adequate cognitive and communication function to sign informed consent, understand the training instruction, use the device, and give adequate feedback 3.1. Exclusion criteria - Having cognitive impairment (score less than 3 points by Thai Mental State Examination (TMSE)) (Appendix C). - Having musculoskeletal problem or cardiovascular disease affecting ability to stand and walk. 28 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 17 - Loss of proprioceptive sense of lower extremity. - Severe spasticity of lower extremity muscles (scale more than 3 point by Modified Asworth Scale: considerable increase in tone; passive movement difficult, affected part is rigid in flexion or extension) (Appendix C). - Having visual problem that was not corrected through eye-glasses. - Having tightness of gastrocnemius. - Having limited range of motion (ROM) in lower extremities. - Lower motor neuron injury with inadequate response to stimulation. Patient s characteristics were summarized in Table 3.1. All patients resembled in both cognitive abilities and physical impairments including the demographic and clinical data. Table 3.1 Characteristics of subjects Subject s characteristics Gender Male : Female Control group (n = 8) 6: FESm group (n = 8) 5:3 FESd group (n = 8) 6: p-value a - Side Right : Left 3:5 3:5 :6 - Type Infarction : Hemorrhage 6: 6: 6: - Age Mean ± SD 5.13 ± ± ± Time since stroke (months) Mean ± SD 5.88 ± ± ± TSME score Mean ± SD 6.63 ± ± ± a : p-value from One-way ANOVA * : Significantly different (p<0.05) 29 Winai Chatthong Materials and Methods / Training procedures Twenty-four subjects who met the inclusion criteria were divided into three groups of eight; 1) control group, ) ES with massed practice (ESm), and 3) ES with distributed practice (ESd). Each group received different one-hour training programs for three times a week for a total period of ten times (4 weeks). At the end of training, knee control improvement was evaluated by assessing the knee angle and knee response time. In the control group, subjects received a standard rehabilitation for 60 minutes by physical therapist. A standard rehabilitation included exercising, promoting self-help activities and using special techniques in order to performed knee control on the hemiparetic leg. These activities were done by the resisted band during standing to reactivate muscle working. Both ES groups received the same standard rehabilitation as the control group for only 30-minute. The ES training program was then applied for 30 minutes. Two x square electrodes were positioned on the thigh muscle groups of affected leg (Fig 3.1a). The active stimulation electrode was placed over the muscle belly of the hamstrings (semi-membranosus) and the indifferent electrode was placed over the medially just distal from the head of the fibular on the same leg. Stimulating pulses were asymmetrical biphasic in order to elicit the muscle contraction only underneath the stimulating electrode. The 30-minute training program for ESm group was divided into 5 sessions. Each session consisted of 5-minute continuous exercise followed by one minute rest period between sessions. The ESd training program consisted of 3 sessions of 5-minute continuous exercise with 5-minute rest in between sessions. Flowchart of the training programs for all three groups was summarized in Fig 3. 30 Fac. of Grad. Studies, Mahidol Univ. F M.Eng.(Biomeedical Engineeering) / 19 a. Inddifferent Eleectrode Acctive Electro ode b. Startting positionn Finnal position Figure 3.1 Preeparation off training (a)) position off electrodess placement,, (b) starting andd final posittion during training andd reponse tiime evaaluation 31 Winai Chatthong Materials and Methods / 0 In the 30-minute ES training program, subject stood on a bathroom scale. The horizontal bar was placed in front of the knee level in order to be the guideline of 15- degree knee flexion position (Fig 3.1b). Subject took weight on the affected leg at least 50% then flexed the knee to the horizontal bar by themselves without trunk bending or heel rising. If the knee flexion could not be performed to reach the bar, subject could activate the stimulator to assist it. While returning to a straight position, subject attempted to control the knee extending smoothly, slowly order to avoid hyper extending the knee. During training the researcher stood at the affected side of subject for safety. 3.3 Assessment procedures Two assessments of knee control performance were evaluated at before and after the training, including knee angle and response time. Post-training assessment was conducted at 1) immediately, ) 15 minutes afterwards, and 3) 4 hours after the training programs had completed (Fig 3.3). a) Knee angle Knee angle was measured as follows. Subjects were asked to wear perforating pants. Three adhesive markers were placed on bony landmarks at greater trochanter, lateral femoral condyle, and lateral malleolus on affected side before assessment started (Fig 3.4). Subjects were instructed to walk independently at their most comfortable speed along 4-meter walkway twice for video recording [96] (Fig 3.5). Snap shots of the video clips were captured by Microsoft Windows Movie Maker in order to select frame of knee angles for kinematic analysis. Then, MATLAB and Scion Image program were used to digitize markers on image that represented degrees of knee angles. Mean error of this method from multiple measurement of the same picture was only 0.1 degree (Appendix E) and this error amount was negligible. 32 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 1 4 patients admitted to clinic of Faculty of Physical Therapy and Applied Movement Science and screened for this study. Randomized (n=4) Control group (n=8) ES groups (n=16) Control group (n=8) 30 minutes of Lower-limb training with conventional physical therapy and knee control training by physical therapist around 30 minutes Subjects have to train 10 times. ESm group (n=8) 30 minutes of Lower-limb training with conventional physical therapy, 30 minutes of Lower-limb training with electrical stimulation ; 5 minutes continuous training and one minute for resting (5 session). Subjects have to train 10 times. Randomized (n= 16) ESd group (n=8) 30 minutes of Lower-limb training with conventional physical therapy, 30 minutes of Lower-limb training with electrical stimulation ; 5 minutes continuous training and 5 minutes for resting. (3 session) Subjects have to train 10 times. Assessment Knee angle during walking, Knee angle during standing (after knee flexion), Response time during standing Pre-training, immediate after training and 15 minutes after resting (all times in training) Assessment Knee angle during walking, Knee angle during standing (after knee flexion), Response time during standing Pre-training, immediate after training and 15 minutes after resting (all times in training) Assessment Knee angle during walking, Knee angle during standing (after knee flexion), Response time during standing Pre-training, immediate after training and 15 minutes after resting (all times in training) Post-training when finish course training exceeding 4 hours Post-training when finish course training exceeding 4 hours Post-training when finish course training exceeding 4 hours Figure 3. Flowchart of the training programs. 33 Winai Chatthong Materials and Methods / Training Resting exceed 4 hours after training 1 60 minutes 3 4 Figure 3.3 The assessment diagram; 1 = pre-training assessment, = immediate post-training assessment, 3 = at 15-minute rest post-training assessment, 4 = 4 hours after the training programs had completed Figure 3.4 The position of marker 34 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 3 4-meter walkway meter Camera Figure 3.5 The top view of camera and walkway in this study The definition of knee angle is shown in Figure 3.6. Positive knee angles represent knee flexion ( θ ) which is the angle between the line joining markers the greater trochanter and lateral femoral condyle. Other one is between the lateral femoral condyle and lateral malleolus. Negative angles indicate knee extension ( θ ). The normal value of knee angle during midstance was reported to be 5-10 degrees [6, 9]. θ = 180 β Greater trochanter β θ Lateral femoral condyle Lateral malleolus β θ 3 Knee flexion Knee extension Figure 3.6 Location of markers and knee angle in the sagittal plane. 1 = Greater trochanter, = Lateral fermoral condyle, 3 = Lateral malleolus 35 Winai Chatthong Materials and Methods / 4 b) Response time of knee control Response time for knee control during standing was evaluated. It is widely used to identify the performance of motor recovery which will be effective in remediation of stroke patients [1, 97]. Subject was informed to stand on two bathroom scales (Fig 3.1b) and took the weight on the affected leg at least 50% of body weight or at the most if 50% was not possible in order to stimulate the natural manner as midstance phase of gait cycle. Then, the subject waited for a bell ring and then flexed the affected knee to the horizontal bar for setting knee flexion at 15 degrees by themselves without trunk bending and heel rising (Fig 3.1b). Response time was recorded by a digital stopwatch. High intratester reliability of response time was shown in Appendix F. 3.4 Statistical Analysis The knee angle and response time were analyzed using the SPSS for Windows. The level of statistically significant difference for all analyses was set at p-value less than 0.05 (p<0.05). The Kolmogorov Smirnov Goodness of Fit test was used to test for the distribution of the data. For normal distribution, the One-way ANOVA was used to compare age, time post onset and TSME score between control and ES groups. ANOVAs with repeated measurement were used to compare knee angle and response time among pre-training and post-trainings. 36 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 5 CHAPTER V RESULTS 4.1 Immediate effect of ES training on Knee Angle and Response Time Immediate effect of different one-hour training programs on knee control improvement was investigated by comparing knee angle ( ) and response time (RT) among all three groups measured at 1) before ( pre, RT pre ), ) immediately after ( im,, RT im ), and 3) 15-minutes after ( 15, RT 15 ) each one-hour training set Knee angle Fig 4.1a and Fig 4.a shows the knee angles during standing and walking, respectively, for all three groups measured at 15 minutes after the one-hour training. At the fist-five training days, knee angles did not change indicating the ineffectiveness of the training programs. Afterward, however, knee angles of ESd group improved gradually after each one-hour training, whereas those of control and ESm group remained the same. These results suggested that only the ESd training program could decrease the degree of hyperextension. The knee angle improvement at immediately post-training ( Δ θ = θ θ ) measured during standing and walking were shown in Fig 4.1b and Fig 4.b, respectively. The positive value represented the reduction of hyperextension. After the 5 th training, im of both ES groups were comparable and more than that of control, indicating the effectiveness of ES training. However, at 15-minute post-training, this improvement of ESm training disappeared whereas that of ESd remained (Fig 4.1c and Fig 4.c). Only the ESd training program could decrease the degree of hyperextension. im im pre 37 Winai Chatthong Results / 6 Anterior Posterior a. Knee angle (degrees) (Ө) min after training Hip 1.00 β Knee 0.00 θ Ankle θ = 180 β Control group (Times) 9 Massed group Distributed group b. c. ( Ө) Knee angle during standing (IM - Pre) Knee angle (degrees) Knee angle (degrees) ( Ө) (Times) Knee angle during standing (15 - Pre) (Times) Figure 4.1 Knee angle during standing on (a) 15-minutes post-training (b) the difference during immediate post-training and pre-training, (c) the difference during 15-minutes post-training and pre-training of control (n=8), the ESm (n=8), and the ESd (n=8) groups in each 10 day. 38 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 7 Anterior Knee angle (degrees) a. (Ө) 15-min after training 0.00 Hip β Knee θ Ankle θ = 180 β Control group b. ( Ө) Massed group 10 (Times) Distributed group c. Knee angle during walking (IM - Pre) 1.0 ( Ө) Knee angle during walking (15 - Pre) 1.0 Knee angle (degrees) Knee angle (degrees) Posterior Response time (Times) (Times) Figure 4. Knee angle during walking on (a) 15-minutes post-training (b) the difference during immediate post-training and pre-training, (c) the difference during 15-minutes post-training and pre-training of control (n=8), the ESm (n=8), and the ESd (n=8) groups in each 10 day. 39 Winai Chatthong Results / 8 Response time measured at 15 minutes after each one-hour training for all three groups was shown in Fig 4.3a. Response time of the control and ESm groups were nearly identical and only slightly improved between trainings. On the other hand, that of ESd group significantly improved after the 5 th training. The ESd training could decrease the response time, thus achieving the motor recovery of knee control. The response time improvements at immediately post-training ( RTim RTim pre) and at 15-minute post-training ( RT15 RT15 pre) were shown in Fig 4.3b and Fig 4.3c, respectively. The negative value indicated the decrease in response time and, therefore, the improvement of knee control. For all three training group, both RTim and RT15 were only slightly negative, implying that the motor response after training not effective enough to motor recovery in the early period. However after the 5 th training, RT15 of ESd group training showed interting results. The prolong performance of response in knee control was presented on the ESd group in particular. The finding suggested that the ESd had a relatively permanent effect. Also, the motor recovery of knee control enhanced excitability facilitation after completing training 15-minute by electrical stimulation with distributed practice. The improving of the motor recovery of knee control, noticeable in Fig 4.4a, implies that there was a decrease in the response time during knee flexion. Fig 4.4b, the result of RT was always near zero. This means that the patient had completely learnt with electrical stimulation program at rehabilitation ward. 40 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 9 a min after training Response time (s) (Times) Control group Massed group Distributed group b. Response time (IM - Pre) c. Response time (15 - Pre) Time (s) Time (s) (Times) (Times) Figure 4.3 Response time during standing in knee flexion on (a) 15-minute post-training (b) the difference during immediate post-training and pre-training, (c) the difference during 15-minute post-training and pre-training of control (n=8), the ESm (n=8), and the ESd (n=8) groups in each 10 day. 41 Winai Chatthong Results / 30 a. b Response time (15 (n+1) -15 (n) ) 0.40 Response time (Pre n+1) -15 (n) ) Time (s) Time (s) (Times) (Times) Control Massed Distributed Control Massed Distributed Figure 4.4 Arithmetic series of response time on (a) the difference arithmetic series at 15-minute post-training (b) the difference during arithmetic series of pre-training and 15-minute post-training of control (n=8), the ESm (n=8), and the ESd (n=8) groups in each 10 day. 4. Overall improvement after completing the training To determine the overall improvement of motor recovery, knee angles and response time were measured at 4 hours after the training programs had completed. Improvements of knee angles and response times within the training group and between groups were evaluated by one-way and two-way ANOVA, repectively. Kolmogorov-Smirnov Goodness of Fit test was also performed and showed normal distribution Control group Either knee angle or response time were not significantly different between before and after the training (Figure 4.5, p>0.05). The means of knee angle and response time after the training program were only slightly promoted. 42 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / ESm group Although, result was no significant difference in the knee angle (Figure 4.5a, p>0.05) between pre and post training, average of knee angle showed some improvement. Response time was significantly improved (Figure 4.5b, p<0.05) for the post training. These results indicated that efficient ES with massed practice could increase response during knee control over standard rehabilitation. a. pre-training post-training Standing Walking Control Massed Distributed Control Massed Distributed 0.00 Knee angle (degrees) (n=8) (n=8) (n=8) b. Response time Time (s) Control Massed Distribute Figure 4.5 Comparison of knee angle and response time within the training group on (a) knee angle during standing and walking for control and ES groups and, (b) response time for control and ES groups. The star indicates when the results obtained in pre (white bars) and post (black bars) training are significantly different (p<0.05). 43 Winai Chatthong Results / 3 Percent change following training was used for comparison in this experiment. Knee angles during standing and walking were computed using a normal knee angle (5 degrees) as a reference [6, 7, 9]. Also the response time, time of post-training was subtracted from that of pre-training. This remaining was time changing, it was then converted to percentage. There was no difference in percent change of knee angle and response time (Figure 4.6, p>0.05) between the control and the ESm group. ESm with standard rehabilitation was only as effective as the standard rehabilitation to improve the knee control of stroke patients. Nevertheless, percent changes in knee angle and response time of ESm group were more than those of control group ESd group The results achieved in the ESd showed a significant enhancement in the knee angle (p<0.05) and response time (p<0.05) when compared between pre and -post trainings (Figure 4.5). That indicated the decrease in the KH and response time during knee flexion. Consequently, the beneficial training of ESd over ESm and standard rehabilitation on performance was recognized at the end of course training. Furthermore, there was significant difference in the percent changes of knee angle and response time between ESm group and control group (Figure 4.6, p<0.05). This meant that the ESd conditions regained better than ESm conditions, especially in a motor control. 44 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 33 a. Standing Walking Percent change in knee angles (%) (n=8) (n=8) Control Massed (n=8) Distributed Control Massed Distributed b. Respo onse time Percent change in time (%) Control Massed Distributt ed Figure 4.6 Percent-change comparison between groups on (a) knee angle during standing and walking (b) responsee time after 4 hours. The star and cross hairs indicate when the results obtained from control and ESd group, ESm and ESd groups were of significant difference (p<0.05), respectively. 45 Winai Chatthong Discussion / 34 CHAPTER VI DISCUSSION This study compared the effectiveness of rehabilitation programs on the motor recovery of stroke patients and showed that electrical stimulation (ES) training was more effective than the standard manual facilitation rehabilitation. Moreover, the study discovered that stimulation parameter of ES training was also critical in promoting the motor recovery. The ESd program was significantly more effective than was the ESm. Before training, subjects characteristics were similar regarding the demographic and clinical data (Table 3.1). Recovering or learning ability in each subject was necessary to consideration. On account of the spontaneous recovery, subjects had onset of stroke more than three months [98]. Therefore, the patient improvement should be due to the training program, not the spontaneous recovery. Besides, cognitive deterioration was also concerned for motor learning and functional recovery in stroke [1]. Subjects were required to take the TMSE examination (Appendix C). Additionally, limited range of motion (ROM) and severe spasticity of lower extremity were contributed to the adaptation or limitation of the knee movement during walking [5]. Modified Ashworth scale was used for screening muscle tone of lower extremity. It could reduce the effect of training. ES has been applied to several applications for motor recovery in individuals after stroke [39]. ES can elicit muscle contraction producing ascending somatosensory feedback sent to the primary cortex [99] and this is not possible by standard manual facilitation rehabilitation [1]. Additionally, ES assisted movement has been shown to suppress the spasticity of the antagonist muscle [ ]. Moreover applying the ES only while patients perform voluntary movement can further improve the motor recovery. This is proven by electromyogram (EMG)-triggered neuromuscular 46 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 35 stimulation [ ]. The cerebral blood flow in the sensory-motor cortex area on the pathologic side was increased [87]. For this study, patients turned on the stimulator only when they try to contract that muscle that is the same as using EMG trigger. In this study, the prolong performance in knee angle and response time indicated achieving of motor recovery. In the immediate effect, knee angle and response time of control and ESm groups revealed similar slight achieving of motor recovery of knee control. This result differs from the literature [39, 87, 89, 94, 99, 101, ] which suggested that patients with ES training recovered more than those with the standard rehabilitation. The ESd group showed higher motor recovery of knee control than either the control or ESm groups. There were four hypotheses to improve knee control after the training. The first was spacing effect. This effect involves producing during repetitive movement [111]. It presented distinct advantage of the ESd over ESm which may be the longer periods of rest in distributed practice condition. Also, this effect was related with ESd. Reactive impedance was the second effect in this study. It mentioned a possible discrepancy between performance and learning during training. This extensive effect can be adjusted by the training chosen [49]. This effect is lessened by a longer rest period. Consequently, the reactive impedance presented in ESm over ESd for this study. It is also precise that good motor recovery improvement in ESd group was because of this effect [11]. The third hypothesis was the psychology literature [113], reminiscence was able to present in ESd group, not the ESm [11]. The advantage of this effect delivered the subjects in ESd group. They had a longer rest period of time in a learning environment. Furthermore it involved mental practice theory [1]. 47 Winai Chatthong Discussion / 36. The last hypothesis that consequentially affected this distinct advantage of the ESd over FESm could be the muscle fatigue. Fatigue is probably the factor of ESm depressing and degrading capable performance and motor recovery [1]. In our study, the average number of repetitions performed of knee control training was 17 in ESm. Hence, after training, result was shown that the partial improved performance then could be depressed earlier because of temporary fatigue from continuous practice [0]. Differently, the average number of repetitions performed was 131 in ESd. For these tasks, distributed practice schedules were preferable. Though ESd training program showed promising results, further studies are under way to validate the effectiveness of this training program. 48 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 37 CHAPTER VII CONCLUSION This study showed that ESd training program promoted the motor recovery significantly better than did either ESm or traditional manual facilitation training. ESd training program was effective to improve knee angle and response time for the kneehyperextended patients. A further study is under way to evaluate the effectiveness and long-term effect of ESd trainng program. 49 Winai Chatthong Clinical relevance and Further study / 38 CHAPTER VIII CLINICAL RELEVANCE AND FURTHER STUDY In rehabilitation, fatigue would be avoided after training on account of performance and learning. The increasing of rest periods could help prevent the fatigue and could enhance learning. In addition, the weight bearing on the affected leg should be carefully considered during ES training. The patient could bear more weight on the affected leg because performing was deeply involved in proprioceptive sense [11]. According to design methodology, it will be interesting to compare outcomes between passive training and functional training with ES. The passive training applies FES in practicing movement while subject does not voluntarily move until finish. Conversely, in the functional training subject does focus in task while ES is stimulating. Nevertheless, previous research revealed that functional training was better than passive training [114] The small sample size of this study has obvious restrictions in generalizing to extensive stroke population. Further studies are needed to enlarge the number of subjects in each group again. Also it will be more effective statistically in type II error. It is also interesting to study the remaining treatment effect in the maintenance phase following the end of intervention by a longitudinal follow-up study. To understand the effects of ES, neuromuscular adaptation should be studied after long term training by specific measurement such as EMG muscle activity, fmri pre-motor area excitability, muscle strengthening, and biomechanics analysis. 50 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 39 REFERENCES 1. Kollen B, Kwakkel G, Lindeman E. Functional recovery after stroke: a review of current developments in stroke rehabilitation research. Rev Recent Clin Trials. 006 Jan;1(1): McDowd JM, Filion DL, Pohl PS, Richards LG, Stiers W. Attentional abilities and functional outcomes following stroke. J Gerontol B Psychol Sci Soc Sci. 003 Jan;58(1):P Greenberg DA, Aminoff MJ, Simon RP. Clinical neurology: Mc Graw-Hill Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 008 Jan 9;117(4):e Stepwise approach to stroke surveillance 005 Oct 1 [cited; Available from: http// 6. Ministry of Public Health. Burden of disease and injuries in Thailand. Priority setting for policy. 00:A Petrilli S, Durufle A, Nicolas B, Pinel JF, Kerdoncuff V, Gallien P. Prognostic factors in the recovery of the ability to walk after stroke. J Stroke Cerebrovasc Dis. 00 Nov-Dec;11(6): Karl J. Sandin, Kristin D. Mason. Manual of Stroke Rehabilitation: Butterworth- Heinemann Dobkin BH. Clinical practice. Rehabilitation after stroke. The New England journal of medicine. 005 Apr 1;35(16): Krakauer JW. Motor learning: its relevance to stroke recovery and neurorehabilitation. Curr Opin Neurol. 006 Feb;19(1): Shumway-Cook A, Woollacott MH. Motor control: Theory and practical applications. ed. New York: Lippincott Williams and Wilkins 001. 51 Winai Chatthong References / Buitrago MM, Schulz JB, Dichgans J, Luft AR. Short and long-term motor skill learning in an accelerated rotarod training paradigm. Neurobiology of learning and memory. 004 May;81(3): Classen J, Liepert J, Wise SP, Hallett M, Cohen LG. Rapid plasticity of human cortical movement representation induced by practice. Journal of neurophysiology Feb;79(): Karni A, Meyer G, Jezzard P, Adams MM, Turner R, Ungerleider LG. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature Sep 14;377(6545): Karni A, Meyer G, Rey-Hipolito C, Jezzard P, Adams MM, Turner R, et al. The acquisition of skilled motor performance: fast and slow experience-driven changes in primary motor cortex. Proc Natl Acad Sci U S A Feb 3;95(3): Liepert J, Terborg C, Weiller C. Motor plasticity induced by synchronized thumb and foot movements. Exp Brain Res Apr;15(4): Rosenbaum DA, Carlson RA, Gilmore RO. Acquisition of intellectual and perceptual-motor skills. Annu Rev Psychol. 001;5: Taub E, Uswatte G, Pidikiti R. Constraint-Induced Movement Therapy: a new family of techniques with broad application to physical rehabilitation--a clinical review. Journal of rehabilitation research and development Jul;36(3): Mathiowetz V, Haugen JB. Motor behavior research: implications for therapeutic approaches to central nervous system dysfunction. Am J Occup Ther Aug;48(8): Schmidt RA, Lee TD. Motor control and learning: A behavioral emphasis. ed. United states of America: Human Kinetics Magill RA. Motor learning: concepts and applications. 5 ed. United States of America: McGraw-Hill Taub E, Morris DM. Constraint-induced movement therapy to enhance recovery after stroke. Curr Atheroscler Rep. 001 Jul;3(4):79-86. 52 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / Burdett RG, Borello-France D, Blatchly C, Potter C. Gait comparison of subjects with hemiplegia walking unbraced, with ankle-foot orthosis, and with Air- Stirrup brace. Phys Ther Aug;68(8): Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Recovery of walking function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil Jan;76(1): Knutsson E, Richards C. Different types of disturbed motor control in gait of hemiparetic patients. Brain Jun;10(): Kaplan PE, Caillient R, Kaplan CP. Rehabilitation of stroke. New York: Butterworth Heinemann Perry J, Garrett M, Gronley JK, Mulroy SJ. Classification of walking handicap in the stroke population. Stroke Jun;6(6): Daly JJ, Ruff RL. Electrically induced recovery of gait components for older patients with chronic stroke. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists. 000 Jul-Aug;79(4): Perry J. Gait analysis Normal and Pathological Function.. New York: Slack Incorporated Morris ME, Matyas TA, Bach TM, Goldie PA. Electrogoniometric feedback: its effect on genu recurvatum in stroke. Arch Phys Med Rehabil. 199 Dec;73(1): Hogue RE, McCandless S. Genu recurvatum: auditory biofeedback treatment for adult patients with stroke or head injuries. Arch Phys Med Rehabil Aug;64(8): Kerrigan DC, Deming LC, Holden MK. Knee recurvatum in gait: a study of associated knee biomechanics. Arch Phys Med Rehabil Jul;77(7): Mulroy S, Gronley J, Weiss W, Newsam C, Perry J. Use of cluster analysis for gait pattern classification of patients in the early and late recovery phases following stroke. Gait Posture. 003 Aug;18(1):114-5. 53 Winai Chatthong References / Jessica Rose, James G. Gamble. Human walking: Williams & Wilking Wang RY. Effect of proprioceptive neuromuscular facilitation on the gait of patients with hemiplegia of long and short duration. Phys Ther Dec;74(1): Paci M. Physiotherapy based on the Bobath concept for adults with post-stroke hemiplegia: a review of effectiveness studies. J Rehabil Med. 003 Jan;35(1): Carr JH, Shepherd RB, eds. Stroke rehabilitation: guidelines for exercise and training to optimize motor skill. London: Butterworth and Heinemann Moreno JC, Brunetti F, Rocon E, Pons JL. Immediate effects of a controllable knee ankle foot orthosis for functional compensation of gait in patients with proximal leg weakness. Med Biol Eng Comput. 008 Jan;46(1): Sheffler LR, Chae J. Neuromuscular electrical stimulation in neurorehabilitation. Muscle Nerve. 007 May;35(5): Peckham PH, Knutson JS. Functional electrical stimulation for neuromuscular applications. Annual review of biomedical engineering. 005;7: Ekholm J, Arborelius UP, Hillered L, Ortqvist A. Shoulder muscle EMG and resisting moment during diagonal exercise movements resisted by weight-andpulley-circuit. Scand J Rehabil Med. 1978;10(4): Bobath B. Adult hemiplegia: evalution and treatment. 3 ed. Oxford: Butterworth and Heineman Lee TD, Swanson LR, Hall AL. What is repeated in a repetition? Effects of practice conditions on motor skill acquisition. Phys Ther Feb;71(): Vearrier LA, Langan J, Shumway-Cook A, Woollacott M. An intensive massed practice approach to retraining balance post-stroke. Gait Posture. 005 Oct;(): Farncombe PM. The Swedish knee cage. Management of the hyperextended hemiplegic knee. Physiotherapy Jan;66(1): de Wit DC, Buurke JH, Nijlant JM, Ijzerman MJ, Hermens HJ. The effect of an ankle-foot orthosis on walking ability in chronic stroke patients: a randomized controlled trial. Clin Rehabil. 004 Aug;18(5):550-7. 54 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / Dingguo Z, Tan Hock G, Ferdinan W, Wei Tech A. Functional electrical stimulation in rehabilitation engineering: a survey. Proceedings of the 1st international convention on Rehabilitation engineering \& assistive technology: in conjunction with 1st Tan Tock Seng Hospital Neurorehabilitation Meeting. Singapore: ACM Rushton DN. Functional electrical stimulation. Physiological measurement Nov;18(4): Mackay S, Morgan P, Datta V, Chang A, Darzi A. Practice distribution in procedural skills training: a randomized controlled trial. Surg Endosc. 00 Jun;16(6): Boyd L, Winstein C. Explicit information interferes with implicit motor learning of both continuous and discrete movement tasks after stroke. J Neurol Phys Ther. 006 Jun;30():46-57; discussion Chen CL, Chen HC, Tang SF, Wu CY, Cheng PT, Hong WH. Gait performance with compensatory adaptations in stroke patients with different degrees of motor recovery. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists. 003 Dec;8(1): Kim CM, Eng JJ. Magnitude and pattern of 3D kinematic and kinetic gait profiles in persons with stroke: relationship to walking speed. Gait Posture. 004 Oct;0(): Barnett HJM, Stein BM, Mohr JP, Yatsu FM. Stroke: pathophysiology, diagnosis, and management. New York: Churchill Livingstone Kisner C, Colby LA. Therapeutic exercise: foundations and techniques. Philadelphia: F.A. Davis company Hintermeister RA, Bey MJ, Lange GW, Steadman JR, Dillman CJ. Quantification of elastic resistance knee rehabilitation exercises. The Journal of orthopaedic and sports physical therapy Jul;8(1): Hostler D, Schwirian CI, Campos G, Toma K, Crill MT, Hagerman GR, et al. Skeletal muscle adaptations in elastic resistance-trained young men and women. Eur J Appl Physiol. 001 Dec;86(): Krebs DE, Jette AM, Assmann SF. Moderate exercise improves gait stability in disabled elders. Arch Phys Med Rehabil Dec;79(1): 55 Winai Chatthong References / Trombly CA. Motor control therapy. Occupational therapy for physical dysfunction. 3 ed. Baltimore: Williams and Wilkins Sabari JS. Motor learning concepts applied to activity-based intervention with adults with hemiplegia. Am J Occup Ther Jun;45(6): Malouin F, Belleville S, Richards CL, Desrosiers J, Doyon J. Working memory and mental practice outcomes after stroke. Arch Phys Med Rehabil. 004 Feb;85(): Page SJ, Levine P, Sisto SA, Johnston MV. Mental practice combined with physical practice for upper-limb motor deficit in subacute stroke. Phys Ther. 001 Aug;81(8): Butefisch C, Hummelsheim H, Denzler P, Mauritz KH. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J Neurol Sci May;130(1): Schmidt RA. Motor control and learning: a behavioral emphasis ed. Illinois: Human Kinetic plublishers Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci. 004;(3-5): Halder P, Sterr A, Brem S, Bucher K, Kollias S, Brandeis D. Electrophysiological evidence for cortical plasticity with movement repetition. Eur J Neurosci. 005 Apr;1(8): Suputtitada A, Suwanwela NC, Tumvitee S. Effectiveness of constraint-induced movement therapy in chronic stroke patients. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 004 Dec;87(1): Shumway-Cook A, Hutchinson S, Kartin D, Price R, Woollacott M. Effect of balance training on recovery of stability in children with cerebral palsy. Dev Med Child Neurol. 003 Sep;45(9): Lai Q, Shea CH, Wulf G, Wright DL. Optimizing generalized motor program and parameter learning. Res Q Exerc Sport. 000 Mar;71(1): Page SJ. Mental practice: a promising restorative technique in stroke rehabilitation. Top Stroke Rehabil. 001 Autumn;8(3):54-63. 56 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / Forrester LW, Wheaton LA, Luft AR. Exercise-mediated locomotor recovery and lower-limb neuroplasticity after stroke. Journal of rehabilitation research and development. 008;45(): Braun C, Schweizer R, Elbert T, Birbaumer N, Taub E. Differential activation in somatosensory cortex for different discrimination tasks. J Neurosci. 000 Jan 1;0(1): Rossini PM, Calautti C, Pauri F, Baron JC. Post-stroke plastic reorganisation in the adult brain. Lancet Neurol. 003 Aug;(8): Schaechter JD. Motor rehabilitation and brain plasticity after hemiparetic stroke. Prog Neurobiol. 004 May;73(1): Carr JH, Shepherd RB. A Motor Relearning Programme for Stroke. London: William Heinemann Medical Books Lepers R, Breniere Y, Maton B. Changes to the gait initiation programme following a running exercise in human subjects. Neuroscience letters Jan ;60(1): Poole JL. Application of motor learning principles in occupational therapy. Am J Occup Ther Jun;45(6): Cirstea CM, Ptito A, Levin MF. Feedback and cognition in arm motor skill reacquisition after stroke. Stroke. 006 May;37(5): Burnside IG, Tobias HS, Bursill D. Electromyographic feedback in the remobilization of stroke patients: a controlled trial. Arch Phys Med Rehabil. 198 May;63(5): Koheil R, Reg PT, Mandel AR. Joint position biofeedback facilitation of physical therapy in gait training. Am J Phys Med Dec;59(6): Dursun E, Dursun N, Alican D. Effects of biofeedback treatment on gait in children with cerebral palsy. Disability and rehabilitation. 004 Jan 1;6(): Olney SJ, Colborne GR, Martin CS. Joint angle feedback and biomechanical gait analysis in stroke patients: a case report. Phys Ther Oct;69(10): Weingarden H, Ring H. Functional electrical stimulation-induced neural changes and recovery after stroke. Eura Medicophys. 006 Jun;4():87-90. 57 Winai Chatthong References / Yan T, Hui-Chan CW, Li LS. Functional electrical stimulation improves motor recovery of the lower extremity and walking ability of subjects with first acute stroke: a randomized placebo-controlled trial. Stroke. 005 Jan;36(1): Hummelsheim H, Maier-Loth ML, Eickhof C. The functional value of electrical muscle stimulation for the rehabilitation of the hand in stroke patients. Scand J Rehabil Med Mar;9(1): Santos M, Zahner LH, McKiernan BJ, Mahnken JD, Quaney B. Neuromuscular electrical stimulation improves severe hand dysfunction for individuals with chronic stroke: a pilot study. J Neurol Phys Ther. 006 Dec;30(4): Fleury M, Lagasse P. Influence of functional electrical stimulation training on premotor and motor reaction time. Perceptual and motor skills Apr;48(): Hara Y. Neurorehabilitation with new functional electrical stimulation for hemiparetic upper extremity in stroke patients. Journal of Nippon Medical School = Nihon Ika Daigaku zasshi. 008 Feb;75(1): Hendricks HT, van Limbeek J, Geurts AC, Zwarts MJ. Motor recovery after stroke: a systematic review of the literature. Arch Phys Med Rehabil. 00 Nov;83(11): Yavuzer G, Geler-Kulcu D, Sonel-Tur B, Kutlay S, Ergin S, Stam HJ. Neuromuscular electric stimulation effect on lower-extremity motor recovery and gait kinematics of patients with stroke: a randomized controlled trial. Arch Phys Med Rehabil. 006 Apr;87(4): Daly JJ, Roenigk KL, Butler KM, Gansen JL, Fredrickson E, Marsolais EB, et al. Response of sagittal plane gait kinematics to weight-supported treadmill training and functional neuromuscular stimulation following stroke. Journal of rehabilitation research and development. 004 Nov-Dec;41(6A): Bogataj U, Gros N, Kljajic M, Acimovic R, Malezic M. The rehabilitation of gait in patients with hemiplegia: a comparison between conventional therapy and multichannel functional electrical stimulation therapy. Phys Ther Jun;75(6): 58 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / Malezic M, Hesse S, Schewe H, Mauritz KH. Restoration of standing, weightshift and gait by multichannel electrical stimulation in hemiparetic patients. Int J Rehabil Res Jun;17(): Lyons GM, Sinkjaer T, Burridge JH, Wilcox DJ. A review of portable FES-based neural orthoses for the correction of drop foot. IEEE Trans Neural Syst Rehabil Eng. 00 Dec;10(4): Ferrante S, Pedrocchi A, Ferrigno G, Molteni F. Cycling induced by functional electrical stimulation improves the muscular strength and the motor control of individuals with post-acute stroke. Europa Medicophysica-SIMFER 007 Award Winner. Eur J Phys Rehabil Med. 008 Jun;44(): Yan TB, Hui-Chan CW, Li LS. [Effects of functional electrical stimulation on the improvement of motor function of patients with acute stroke: a randomized controlled trial]. Zhonghua Yi Xue Za Zhi. 006 Oct 10;86(37): Stuberg WA, Colerick VL, Blanke DJ, Bruce W. Comparison of a clinical gait analysis method using videography and temporal-distance measures with 16- mm cinematography. Phys Ther Aug;68(8): Korner-Bitensky N, Mayo NE, Kaizer F. Change in response time of stroke patients and controls during rehabilitation. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists Feb;69(1): Studenski SA, Wallace D, Duncan PW, Rymer M, Lai SM. Predicting stroke recovery: three- and six-month rates of patient-centered functional outcomes based on the orpington prognostic scale. J Am Geriatr Soc. 001 Mar;49(3): Khaslavskaia S, Sinkjaer T. Motor cortex excitability following repetitive electrical stimulation of the common peroneal nerve depends on the voluntary drive. Exp Brain Res. 005 May;16(4): Bakhtiary AH, Fatemy E. Does electrical stimulation reduce spasticity after stroke? A randomized controlled study. Clin Rehabil. 008 May;(5): Dimitrijevic MR. Clinical practice of functional electrical stimulation: from "Yesterday" to "Today". Artif Organs. 008 Aug;3(8): 59 Winai Chatthong References / Lima MO, Pupio SLF, Takeshi TdFS, Regina-Ribeiro S, Tortoza C, Gomes- Lucareli J, et al. [Effect of neuromuscular electrical stimulation and isotonic exercises in flexor and extensor muscles of knee of hemiplegic patients]. Revista de neurologia. 008 Feb 1-15;46(3): Mally J, Dinya E. Recovery of motor disability and spasticity in post-stroke after repetitive transcranial magnetic stimulation (rtms). Brain research bulletin. 008 Jul 1;76(4): Cauraugh JH, Kim SB, Summers JJ. Chronic stroke longitudinal motor improvements: cumulative learning evidence found in the upper extremity. Cerebrovasc Dis. 008;5(1-): Page SJ, Levine P. Back from the brink: electromyography-triggered stimulation combined with modified constraint-induced movement therapy in chronic stroke. Arch Phys Med Rehabil. 006 Jan;87(1): Cauraugh JH, Kim SB, Duley A. Coupled bilateral movements and active neuromuscular stimulation: intralimb transfer evidence during bimanual aiming. Neuroscience letters. 005 Jul 1-8;38(1-): Daly JJ, Roenigk K, Holcomb J, Rogers JM, Butler K, Gansen J, et al. A randomized controlled trial of functional neuromuscular stimulation in chronic stroke subjects. Stroke. 006 Jan;37(1): Janssen TW, Beltman JM, Elich P, Koppe PA, Konijnenbelt H, de Haan A, et al. Effects of electric stimulation-assisted cycling training in people with chronic stroke. Arch Phys Med Rehabil. 008 Mar;89(3): Knutson JS, Hisel TZ, Harley MY, Chae J. A Novel Functional Electrical Stimulation Treatment for Recovery of Hand Function in Hemiplegia: 1- Week Pilot Study. Neurorehabil Neural Repair. 008 Sep Thrasher TA, Popovic MR. Functional electrical stimulation of walking: function, exercise and rehabilitation. Ann Readapt Med Phys. 008 Jul;51(6): Cepeda NJ, Pashler H, Vul E, Wixted JT, Rohrer D. Distributed practice in verbal recall tasks: A review and quantitative synthesis. Psychol Bull. 006 May;13(3): Whitley JD. Effects of practice distribution on learning a fine motor task. Research quarterly Dec;41(4): 60 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / Bohan M, Pharmer JA, Stokes AF. When does imagery practice enhance performance on a motor task? Perceptual and motor skills Apr;88(): Santos FM, Rodrigues RG, Trindade-Filho EM. [Physical exercise versus exercise program using electrical stimulation devices for home use]. Rev Saude Publica. 008 Feb;4(1):117-. 61 Winai Chatthong Appendix / 50 APPENDIX 62 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 51 APPENDIX A THE ETHICAL COMMITTEE ON RESEARCH INVOLVING HUMAN SUBJECT 63 Winai Chatthong Appendix / 5 APPENDIX B.1 CONSENT FORM ว นท...เด อน...พ.ศ... ข าพเจ า...อาย...ป อาศ ยอย บ านเลขท...หม... หม บ าน/อาคาร...แขวง/ต าบล...เขต/อ าเภอ...จ งหว ด... ขอแสดงเจตนาย นยอมเข าร วมโครงการว จ ยเร อง การศ กษาว ธ กระต นไฟฟ าเพ อฟ นฟ ผ ป วย โรคหลอดเล อดสมองโดยใช อาการเข าแอ น โดยข าพเจ าได ร บทราบเก ยวก บรายละเอ ยดของโครงการด งต อไปน การศ กษาคร งน ม ว ตถ ประสงค เพ อศ กษาศ กษาการเร ยนร การควบค มเข าในเท าท ร บน าหน กภายหล งการใช เคร องกระต นไฟฟ าในการเด นของผ ป วยอ มพาตคร งซ ก ในกรณ ท ผลการศ กษาคร งน เป นไปในทางท ด สามารถน าการฝ กการควบค มข อเข า เพ อแก ป ญหาการเด นเข าแอ นในผ ป วยอ มพาตคร งซ กไปประย กต ใช ในทางคล น กกายภาพบ าบ ดและ การออกแบบทางว ศวกรรม การศ กษาคร งน ไม ก อให เก ดความเส ยงหร ออ นตรายใดๆต อผ เข าร วม การศ กษา โดยตลอดการศ กษาผ เข าร วมการศ กษาจะอย ภายใต การด แลอย างใกล ช ดของผ ว จ ย หากผ ว จ ยม ข อม ลเพ มเต มท งด านประโยชน และโทษท เก ยวข องก บการว จ ยน ผ ว จ ยจะแจ ง ให ข าพเจ าทราบอย างรวดเร วโดยไม ป ดบ ง ข าพเจ าม ส ทธ ท จะของดการเข าร วมโครงการว จ ยโดย ไม ต องแจ งให ทราบล วงหน า โดยการงดการเข าร วมการว จ ยน จะไม ม ผลกระทบต อการได ร บบร การ หร อการร กษาท ข าพเจ าจะได ร บประการใด ข าพเจ าได ร บทราบข อม ลของโครงการข างต นและได ซ กถามผ ว จ ยจนหมดข อสงส ย โดยตลอด และข าพเจ าย นยอมท จะเข าร วมในโครงการด งกล าว โดยขอให ผ ว จ ยงดการเป ดเผยช อ ประว ต ตลอดจนข อม ลท เก ยวข องก บข าพเจ าแก ผ อ นได ร บทราบ ยกเว นข อม ลในร ปสร ปผลการว จ ย หากข าพเจ าไม สามารถเซ นย นยอมเองได ข าพเจ าอน ญาตให ญาต ของข าพเจ าเป นผ เซ นย นยอมแทน ข าพเจ าได ลงช อ...ผ ป วย/ญาต ( ) ลงช อ...ห วหน าโครงการว จ ย ( ) ลงช อ...พยาน ( ) 64 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 53 APPENDIX B. PARTICIPANT INFORMATION SHEET (เอกสารช แจงผ เข าร วมการว จ ย) ในเอกสารน อาจม ข อความท ท านอ านแล วย งไม เข าใจ โปรดสอบถามห วหน าโครงการว จ ย หร อผ แทน ให ช วยอธ บายจนกว าจะเข าใจด ท านอาจจะขอเอกสารน กล บไปอ านท บ านเพ อปร กษาหาร อก บญาต พ น อง เพ อนสน ท แพทย ประจ าต วของท าน หร อแพทย ท านอ น เพ อช วยในการต ดส นใจเข าร วม การว จ ย ช อโครงการ การฝ กควบค มเข าข างร บน าหน กด วยเคร องกระต นไฟฟ าในผ ป วยอ มพาต คร งซ ก ห วหน าโครงการ นายว น ย ฉ ตรทอง สถานท ว จ ย โครงการจ ดต งคณะกายภาพบ าบ ดและว ทยาศาสตร การเคล อนไหวประย กต ช น 5 มหาว ทยาล ยมห ดล เช งสะพานป นเกล า กร งเทพฯ ผ ให ท น ไม ม โครงการว จ ยน ท าข นเพ อศ กษาผลการเปล ยนแปลงการควบค มข อเข าของขาข างท ร บน าหน ก ขณะเด นในผ ป วยอ มพาตคร งซ ก ภายหล งการฝ กด วยเคร องกระต นไฟฟ าโดยม การฝ กแบบช วงเวลา ฝ กนานกว าช วงเวลาพ ก และช วงเวลาฝ กเท าก บช วงเวลาพ ก ซ งจะม ประโยชน ท คาดว าจะได ร บค อ น าผลการศ กษาไปประย กต ใช ทางคล น กในการร กษาผ ป วยอ มพาตคร งซ กเพ อแก ป ญหาการเด นเข า แอ น และการออกแบบทางว ศวกรรม หากผลการศ กษาพบว าการฝ กโดยใช เคร องกระต นไฟฟ า สามารถท าให ผ ป วยควบค มข อเข าขณะเด นได ด ข น ผ ป วยสามารถน าไปฝ กเองท บ านได เพ อเป นการ ประหย ดเวลาและลดค าใช จ าย และผ ป วยสามารถฝ กได ด วยตนเองโดยข นตอนการฝ กไม ย งยาก ท านได ร บเช ญให เข าร วมการว จ ยน เพราะท านเป นโรคหลอดเล อดสมองคร งแรก ซ งม ระยะ เวลาการเก ดโรคมากกว า 3 เด อน สามารถเด นได ด วยตนเองโดยไม ต องพย งหร อใช เคร องช วยเป น ระยะทางอย างน อย 4 เมตร และม อาการเข าแอ นขณะเด นในช วงท ขาข างอ อนแรงร บน าหน ก และ การว จ ยน ท าข นเพ อเป นทางเล อกใหม ท จะน ามาใช ร กษาอาการเข าแอ นขณะเด นในผ ป วยอ มพาตคร งซ ก จะม ผ เข าร วมการว จ ยน ท งส น 4 คน ระยะเวลาท จะท าการว จ ยท งส นเด อนต ลาคม 550 ถ ง เด อนม นาคม 551 65 Winai Chatthong Appendix / 54 เม อท านเข าร วมการว จ ยแล วส งท ท านจะต องปฏ บ ต ตามข นตอนการด าเน นการว จ ยด งต อไปน 1. ข นตอนการเตร ยมการ ผ เข าร วมการว จ ยท กท านจะได ร บการซ กประว ต และตรวจร างกาย เช น ประเม นการร บ ความร ส ก ความต งต วของกล ามเน อและการเคล อนไหวของร างกายบร เวณขา ประเม นความสามารถ ในการจ าและการเร ยนร ตามแบบทดสอบสมรรถภาพสมองของไทย ผ ว จ ยจะอธ บายว ตถ ประสงค, ข นตอนการว จ ย, ประโยชน ของการว จ ย และผ เข าร วมว จ ย ลงนามในใบย นยอมเข าร วมว จ ย. ข นตอนการเก บข อม ล ผ เข าร วมการว จ ยจะได ร บการประเม นการเด นด วยการถ ายภาพว ด โอจากกล องด จ ตอลก อน การฝ กด วยเคร องกระต นไฟฟ า หล งการฝ กด วยเคร องกระต นไฟฟ าท นท และหล งการฝ กด วย เคร องกระต นไฟฟ า 5, 10, 15 นาท และคร งส ดท ายเม อส นส ดการฝ กหล งจาก 4 ช วโมงโดย ผ เข าร วมว จ ยจะสวมกางเกงท จ ดเตร ยมไว ให และต ดเคร องหมายท ข อสะโพก ข อเข าและข อเท าในขา ข างท อ อนแรง จากน นผ เข าร วมการว จ ยเด นบนทางเด นท จ ดเตร ยมไว ให ด วยความเร วปกต เป น ระยะทาง 4 เมตร จ านวน รอบ ขณะท บ นท กภาพการเด น ผ ว จ ยจะท าการบ นท กเวลาท ใช ในการ เด นไปพร อมก น เม อเสร จจากการเด นผ เข าร วมการว จ ยจะมาย นบนเคร องช งน าหน กท จ ดเตร ยมไว แล วงอห วเข าไปแตะก บแท นท ก าหนดไว เม อได ย นส ญญาณกระด ง จ านวน รอบ ขณะท บ นท กภาพการงอห วเข า ผ ว จ ยจะบ นท กเวลาท ใช งอห วเข าไปพร อมๆก น 3. ข นตอนการฝ ก ผ เข าร วมการว จ ยจะได ร บการฝ กเพ อควบค มข อเข าด วยเคร องกระต นไฟฟ า โดยผ เข าร วม การศ กษาจะต องย นฝ กบนเคร องช งน าหน ก ต ว ปลายเท าเหย ยบบนเคร องช งน าหน กข างละต ว ผ ว จ ยต ดแผ นน าไฟฟ าไว ท หล งต นขาในข างท อ อนแรง จากน นให ผ เข าร วมการว จ ยท งน าหน กมาย ง ขาข างท อ อนแรงให มากกว าคร งหน งของน าหน กต ว แล วกดสว ตช เพ อเป ดเคร องกระต นเพ อช วยใน การงอ แล วจ งงอเข าช า ๆ ประมาณ 15 องศา ไปย งเป าหมายท ก าหนดไว ให และค อย ๆ เหย ยดเข า กล บช าๆโดยพยายามควบค มไม ให เข ากระต กหร อแอ นไปด านหล ง การฝ กใช เวลา 30 นาท โดยจะ แบ งเป น แบบ ในแบบแรกฝ ก 5 นาท พ ก 1 นาท ท าท งหมด 5 รอบ ในแบบท ฝ ก 5 นาท พ ก 5 นาท ท าท งหมด 3 รอบ การศ กษาว จ ยคร งน ไม ม อ นตรายใด ๆ ต อผ เข าร วมการศ กษา เน องจากผ ว จ ยจะคอยด แลอย าง ใกล ช ดตลอดระยะเวลาการศ กษา อ กท งม การป องก นการล มขณะฝ กโดยผ ว จ ยจะอย ทางร างกายด าน 66 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 55 ท อ อนแรง ผ เข าร วมการศ กษาสามารถพ กได และผ ว จ ยจะเด นอย ด านหล งเพ อคอยด แลขณะท ผ เข าร วมการศ กษาเด นในข นตอนการประเม น ขณะท าการว จ ยหากผ เข าร บการศ กษาม อาการ ผ ดปกต จะย ต การฝ กท นท อน งในสถานท ท ท าการว จ ยเป นอาคารซ งม น กศ กษาผ ท า ว จ ยกล มอ น ๆ... และอาจารย ทางกายภาพบ าบ ดท ปฏ บ ต งานอย ในบร เวณใกล เค ยง กรณ ท เก ดเหต ส ด ว ส ยสามารถขอ ความช วยเหล อได ตลอดเวลา ผ เข าร วมการศ กษาสามารถต ดต อผ ว จ ย ค อ นายว น ย ฉ ตรทอง ได ตลอดเวลา หากม ข อสงส ยหร อป ญหาท เบอร โทรศ พท หากท านไม เข าร วมในโครงการการว จ ยน ท านก จะได ร บการตรวจ และร กษาโรคของท าน ตามว ธ การท เป นมาตรฐาน การว จ ยน ไม ม ค าตอบแทนท จะได ร บและค าใช จ ายท ผ เข าร วมการว จ ยจะต องร บผ ดชอบใด ๆ หากม ข อม ลเพ มเต มท งด านประโยชน และโทษท เก ยวข องก บการว จ ยน ผ ว จ ยจะแจ งให ทราบโดยรวดเร วไม ป ดบ ง ข อม ลส วนต วของผ เข าร วมการว จ ยจะถ กเก บร กษาไว ไม เป ดเผยต อสาธารณะเป นรายบ คคล แต จะรายงานผลการว จ ยเป นข อม ลส วนรวม ข อม ลของผ เข าร วมการว จ ยเป นรายบ คคลอาจม คณะ บ คคลบางกล มเข ามาตรวจสอบได เช น สถาบ น หร อองค กรของร ฐท ม หน าท ตรวจสอบ, คณะกรรม การจร ยธรรมฯ เป นต น ผ เข าร วมการว จ ยม ส ทธ ถอนต วออกจากโครงการว จ ยเม อใดก ได โดยไม ต องแจ งให ทราบ ล วงหน า และการไม เข าร วมการว จ ยหร อถอนต วออกจากโครงการว จ ยน จะไม ม ผลกระทบต อการ บร การและการร กษาท สมควรจะได ร บแต ประการใด หากท านได ร บการปฏ บ ต ท ไม ตรงตามท ได ระบ ไว ในเอกสารช แจงน ท านจะสามารถแจ งให ประธานคณะกรรมการจร ยธรรมฯ ทราบได ท ส าน กงานคณะกรรมการส ทธ มน ษยชนเก ยวก บการ ทดลองในมน ษย มหาว ทยาล ยมห ดล กองบร หารงานว จ ย ส าน กงานอธ การบด มหาว ยาล ยมห ดล โทรศ พท โทรสาร หร อต ดต อทาง ข าพเจ าได อ านรายละเอ ยดในเอกสารน ครบถ วนแล ว ลงช อ... (...) ว นท... 67 Winai Chatthong Appendix / 56 APPENDIX C PHYSICAL EXAMINATION (แบบฟอร มการตรวจร างกาย) เลขท... ว นท... ช อ นามสก ล..เพศ ว นเก ด อาย. ป น าหน ก.. ก โลกร ม ส วนส ง..... เซนต เมตร ท อย บ านเลขท.หม.. แขวง/ต าบล เขต/อ าเภอ.. จ งหว ด เบอร โทรศ พท โรคประจ าต ว อ ตราการเต นห วใจ คร งต อนาท ความด นโลห ต..ม ลล เมตรปรอท ว นท เก ดโรค. ระยะเวลาการเก ดโรค. ต าแหน งรอยโรค... อ มพาตซ ก ซ าย ขวา ชน ดของโรคหลอดเล อดสมอง สมองขาดเล อด เส นเล อดสมองแตก คะแนนรวมแบบทดสอบสภาพสมองของไทย (TMSE). คะแนน 68 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 57 Physical examination Lower extremities motor assessment 1. Muscle tone 1.1 Hip muscle group Left Right flexor extensor abductor adductor external rotator internal rotator 1. Knee muscle group flexor extensor 1.3 Ankle muscle group dorsiflexor plantarflexor invertor evertor Muscle tone (Modified Ashworth Scale for grading spasticity) 0 no increase in muscle tone 1 slight increase, manifested by a catch and resistance at the end of range of motion when the affected part is moved in flexion or extension 1+ slight increase, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM more marked increase through most of the ROM, but parts easily moved 3 considerable increase, passive movement difficult 4 affected parts rigid in flexion or extension 69 Winai Chatthong Appendix / 58. Joint range of motion (Passive range of motion).1 Hip joint Left Right flexion/extension abduction/adduction internal/external rotation. Knee joint flexion/extension.3 Ankle joint dorsiflexion/plantarflexion 3. Proprioceptive sense 3.1 Hip joint normal impaired 3. Knee joint normal impaired 3.3 Ankle joint: normal impaired 70 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 59 แบบทดสอบสภาพสมองของไทย (TMSE) 1. Orientation การร บร (6 คะแนน) คะแนน (1) ว นน ว นอะไรของส ปดาห (จ นทร อ งคาร พ ธ พฤห ส ฯลฯ)... (1) ว นน ว นท เท าไหร... (1) เด อนน เด อนอะไร... (1) ขณะน เป นช วง (ตอน) ไหนของว น (เช า เท ยง บ าย เย น)... (1) ท น ท ไหน (บร เวณท ตรวจ)... (1) คนท เห นในภาพน ม อาช พอะไร (ภาพอย ด านหล ง).... Registration การจดจ า (3 คะแนน) ผ ทดสอบบอกช อของ 3 อย าง โดยพ ดห างก น คร งละ 1 ว นาท (ต นไม รถยนต ม อ) เพ ยงคร งเด ยวแล วจ งให ผ ถ กทดสอบบอกให ครบตามท ผ ทดสอบบอกในคร งแรก ให 1 คะแนน ในแต ละค าตอบท ตอบถ ก * หมายเหต หล งจากให คะแนนแล วให บอกซ าจนผ ถ กทดสอบจ าได ท ง 3 อย าง และบอกให ผ ถ กทดสอบทราบว าส กคร จะกล บมาถามใหม (1) ต นไม... (1) รถยนต... (1) ม อ Attention ความใส ใจ (5 คะแนน) ให บอกว นอาท ตย -ว นเสาร ย อนหล งให ครบส ปดาห (ให ตอบซ าได 1 คร ง) (1) ศ กร... (1) พฤห สบด... (1) พ ธ... (1) อ งคาร... (1) จ นทร Calculation การค านวณ(3 คะแนน) ให ค านวณ ไปเร อยๆ 3 คร ง (ให 1 คะแนน ในแต ละคร งท ตอบถ กใช เวลาค ดในแต ละ ช วงค าตอบไม เก น 1 นาท หล งจากจบค าถาม) ถ าผ ถ กทดสอบไม ตอบค าถามท 1 ให ต งเลข 93-7 ลองท าในการค านวณคร งต อไป และ 86-7 ในคร งส ดท ายตามล าด บ 71 Winai Chatthong Appendix / 60 (1) (1) (1) Language ด านภาษา (10 คะแนน) (1) ผ ทดสอบช ไปท นาฬ กาข อม อ แล วถามผ ถ กทดสอบว าโดยท วไป เราเร ยกส งน ว าอะไร (นาฬ กา)... (1) ผ ทดสอบช ไปท เส อของตนเองแล วถามผ ถ กทดสอบว าโดยท วไป เราเร ยกส งน ว าอะไร (เส อ, ผ า)... (1) ผ ทดสอบบอกผ ถ กทดสอบว า จงฟ งประโยคต อไปน ให ด แล วจ าไว จากน นให พ ด ตาม ยายพาหลานไปซ อขนมท ตลาด... จงท าตามค าส งต อไปน (ม 3 ข นตอนค าส ง) ให ผ ทดสอบพ ดต อก นไปให ครบประโยคท ง 3 ข นตอนให คะแนนข นตอนละ 1 คะแนน (1) หย บกระดาษด วยม อขวา... (1) พ บกระดาษเป นคร งแผ น... (1) แล วส งกระดาษให ผ ตรวจ... (1) ให ผ ถ กทดสอบอ านแล วท าตาม หล บตา (ข อความอย ด านหล ง)... () จงวาดภาพต อไปน ให เหม อนต วอย างมากท ส ด เท าท ท านจะสามารถท าได... (1) กล วยก บส มเหม อนก นค อเป นผลไม แมวก บส น ขเหม อนก นค อ... (เป นส ตว, เป นส งม ช ว ต) Recall การระล กได (3 คะแนน) ส งของ 3 อย างท บอกให จ าเม อส กคร ม อะไรบ าง (1) ต นไม... (1) รถยนต... (1) ม อ... รวม... 72 Fac. of Grad. Studies, Mahidol Univ. M.Eng.(Biomedical Engineering) / 61 หล บตา Train the Brain Forum (Thailand) Siriraj Hosp. Gaz. Vol. 45 No. 6 June 1993 ( ) กล มฟ นฟ สมรรถภาพสมอง สารศ ร ราช ป ท 45 ฉบ บท 6ม ถ นายน ( ) 536 |

Blockers บล อกซ ม ว นพรอมป วนน เต มเร อง
กระทู้ที่เกี่ยวข้อง
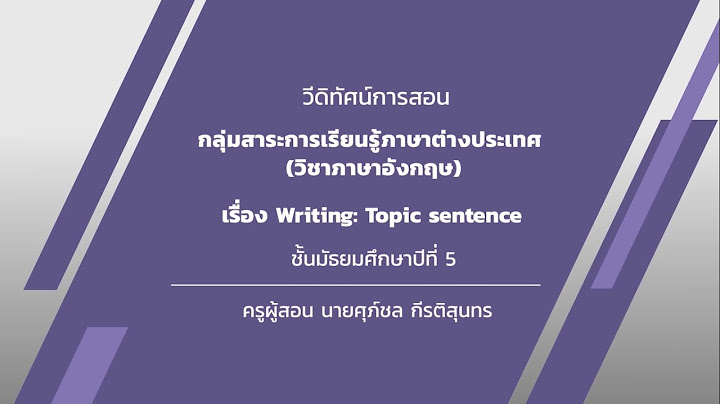











ลิขสิทธิ์ © 2024 th.ketajaman Inc.